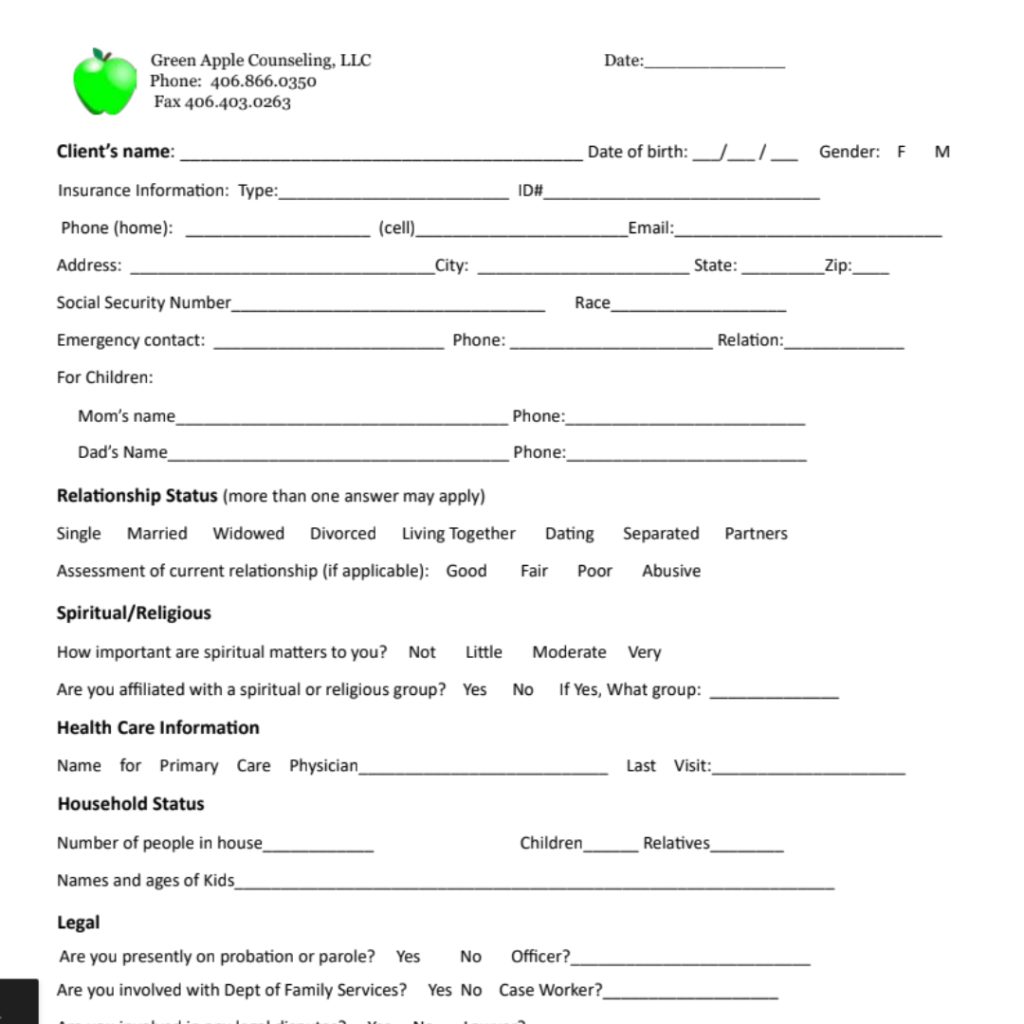
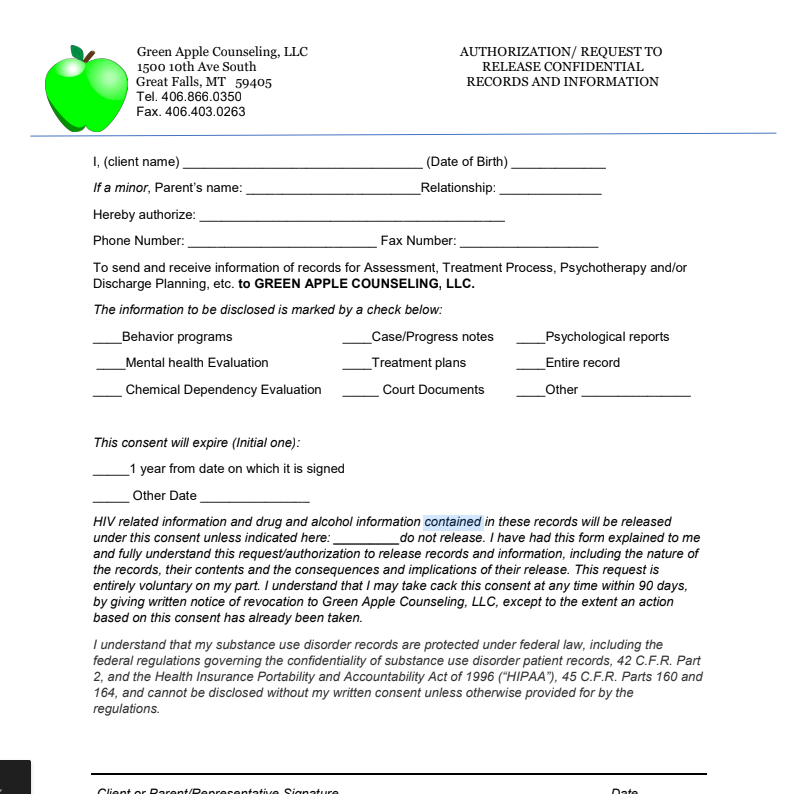
Forms Grievance Name of Grievant(first and last) * Date of Grievance * Client of Green Apple * Phone Number * Statement of Grievance * Relief Sought: * Request Meeting * Yes No Meeting Date * Grievant Signatures * Date * Received By * Date * Rectified Yes If yes, explain Rectified No If no, explain Grievant Signature * Date * Green Apple Director * Date * Submit If you are human, leave this field blank. Physical Form List Mental Health Form Packet Mental Health SUD Packet Prime 4 Life Packet Release of Information